


Ischemic Stroke analysis
Vaccine-related safety signals were detected
Hebrew version גרסה בעברית
Key Points
Data source: Clalit Health Fund, 4.8 million members (FOIA)
Ischemic Stroke (IS) : 2021 - 13% increase, 2022 - 20% increase (vs. 2017-2020 avg.)
IS in babies & children: In 2022 cases increased 2.2-fold compared to previous years. Constant rise in events during 2021, peak was March 2022.
CDC & FDA’s notice on IS safety signal - update
Two known mechanisms by which mRNA vaccines could cause IS
Vaccinated vs. Unvaccinated - explicit increase in IS cases in Vaccinated during second booster rollout
Following our previous post on cardiac arrests, based on data from Clalit Health Fund (4.8 million members as of 2022), we are now publishing ischemic stroke (IS) analysis, also based on Freedom Of Information Act data from Clalit. The data also includes vaccination status. See Reference for an explanation on Ischemic Stroke, source files and ICD-9 codes used.
Clalit noted that the data comes from all of Clalit’s hospitals and for all of Clalit’s members including other hospitals. This may indicate that the total population covered is larger than Clalit’s own members. Due to this, incidence rates were not calculated. (For reference: The yearly growth in Israel’s population is ~1%-2% and is generally insignificant when testing for large-scale safety signals. Furthermore, a steady change in population would be noticeable in the graph)
Death entries include death at any time after the event, including after release from hospital
Clalit added its standard disclaimers (see the clarifications in this post for example). Additionally, they stated that there may be minor differences between age-grouped totals and monthly/yearly totals due to missing age data.
Ischemic Stroke yearly data


Looking at the yearly no. of Ischemic Stroke events, 2017-2020 was chosen as baseline as it appears quite steady (apart from 2019) with less than 1% yearly rise. 2021 exhibits a 13% increase, and 2022 exhibits a 20% increase, or approx. 2000 total excess cases 2021-2022 (calculated using data we received, not total population). The graph above is not adjusted for the growth in population, but the Israeli National Stroke Registry’s 2020 report, which is adjusted, shows a relatively steady, slight drop of the acute stroke rate 2015-2020, further emphasizing the trend reversal we observed in 2021-2022. The Stroke Registry has not yet published 2021-2022 reports.

Another observation from the Ischemic Stroke Events and Deaths graph is that the ratio of IS cases (top graph, Blue) to deaths (Red) shows a steady drop, from 47% down to 17%. This 64% improvement in survival rate, which is supposedly encouraging and began in 2018 or possibly earlier, seems too sharp to be explained merely by ‘advancements in medicine and treatment protocols’. The most extreme example was in the 100+ age group: In 2017 there were 40 IS events and 17 deaths (43% ratio) ; In 2022 there were 51 events and merely 4 deaths (8% ratio) - an 81% improvement. IS deaths may have been misclassified.
Ischemic Stroke monthly data

The available monthly data, which only covers 2021-2022, raises serious questions. There are three months of elevated no. of cases May-July 2021 (compared to avg. monthly rate 2017-2020 of 506 cases). Three months later, a 20% rise within one month (Oct.-Nov. 2021) signifies the beginning of a ‘new, elevated norm’ of 620 avg. monthly cases, ongoing for almost a year, Nov. 2021 to Sep. 2022. The elevated average is 22% higher compared to 2017-2020 monthly avg. The drop in cases on Oct.-Dec. 2022 further supports the theory that this is not a natural rise in cases, a seasonal phenomenon, nor pop. size increase. The graph does not fit the Covid-19 waves, nor vaccine schedule.
Another disturbing graph is the no. of IS cases at ages 0-10 :
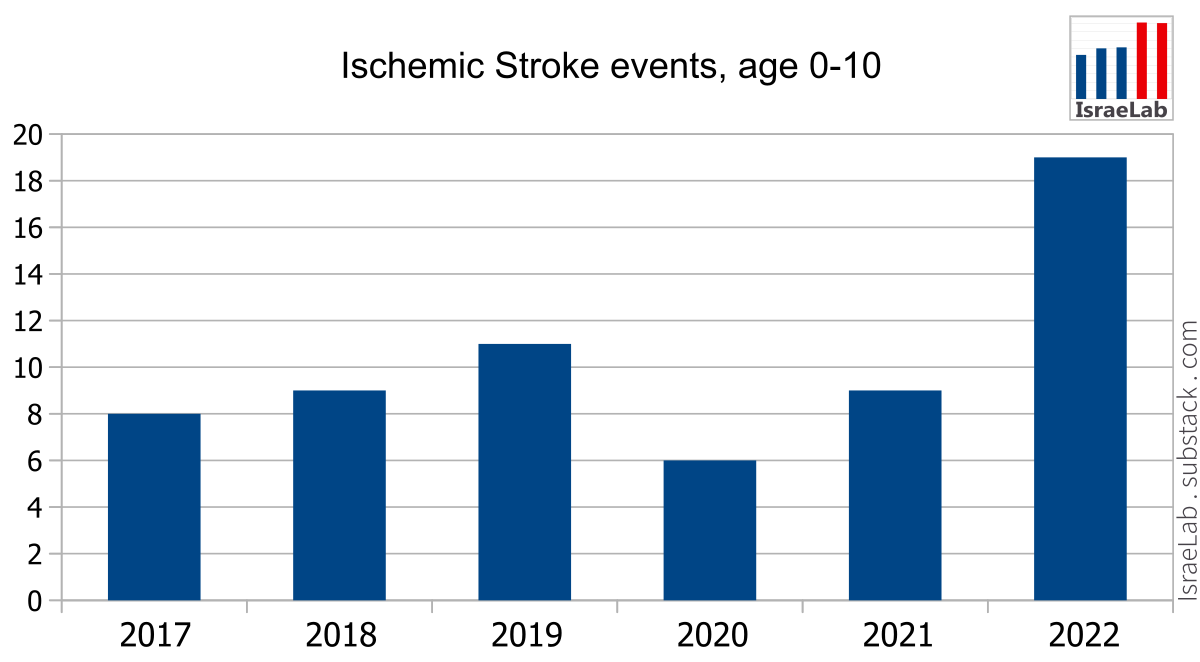
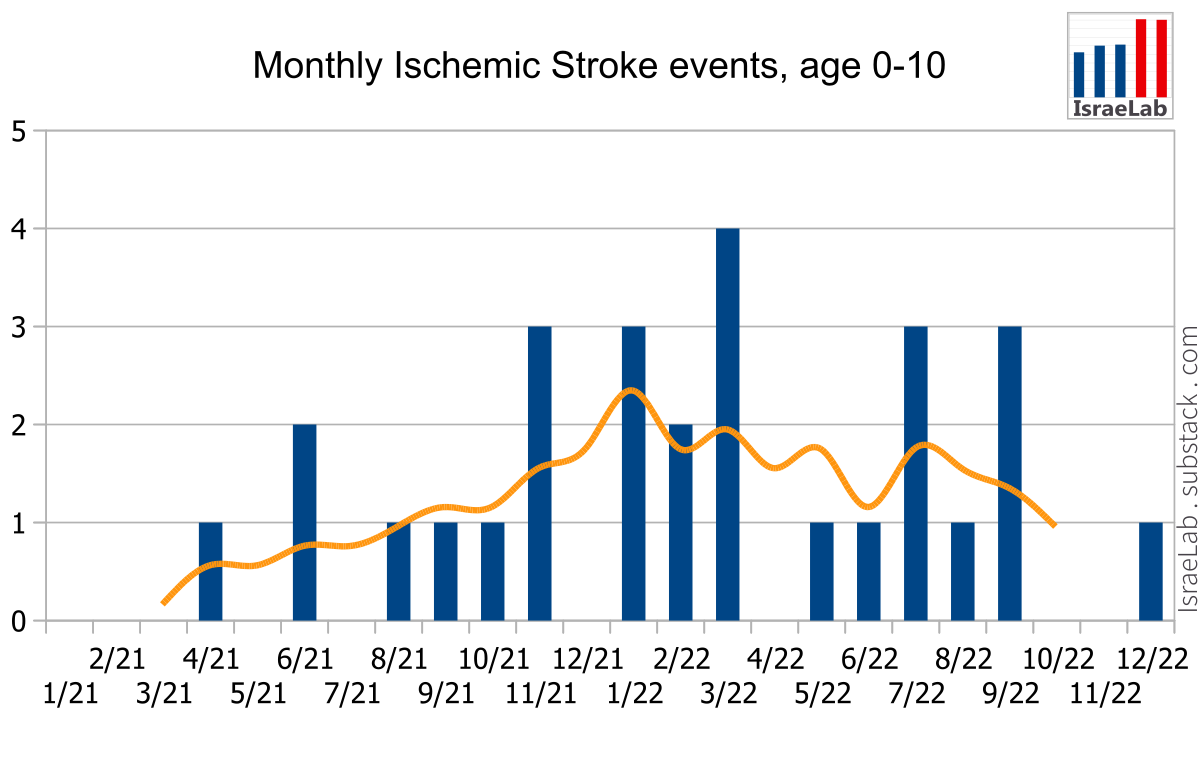
IS is very rare in young ages (0-10). It could never be detected in clinical trials, only in retrospective studies. According to the data from Clalit, the 2017-2020 baseline average is 0.7 events/month, yet the 5-month moving average (Orange line) shows beyond doubt that there is a major increase in IS in children. In 2022 cases increased 2.2-fold compared to previous years. The peak was on March 2022 . Since the sharp rise in IS cases in 2022 does not appear at the adjacent age group (11-20), a possible explanation is that excess IS cases occurred in newborns and babies, for example due to maternal vaccination via breastfeeding: Traces of mRNA vaccines were found in EBM (1) (2), and the effect on newborns has not been thoroughly researched yet. Currently there is no evidence to support this theory. We do not have more detailed age data.
Regarding IS death in young people, in contrary to earlier years, in 2021-2022 there were no deaths at all due to IS under the age of 30, according to Clalit’s data.
CDC & FDA Ischemic Stroke safety signal
On Jan. 13, 2023 the CDC and FDA identified a preliminary COVID-19 vaccine safety signal regarding Ischemic Stroke for persons aged 65 years and older who received the updated (bivalent) Pfizer-BioNTech COVID-19 vaccine, within 21 days of vaccination. Knowing the CDC and FDA, they would not have made a public statement unless there was very clear evidence (at the time) of correlation between the vaccine and stroke cases.
The bivalent vaccine was approved in Israel on July 2022 (prior to FDA approval) (3) (4) and in the US on August 2022, partly based on Israeli health officials’ positive reports. The safety signal appeared later, on the Vaccine Safety Datalink (VSD), a collaborative project between CDC and 9 integrated healthcare organizations across the USA.
On May 31, 2023 the CDC published a statement (see presentation from April 19, 2023) and declared that the initial finding has decreased, and Scientists believe factors other than vaccination might have contributed to the initial finding.
Regarding the CDC’s safety signal, we do not have information specifically concerning those who took the bivalent vaccine. We did not observe a rise in total IS cases* following the bivalent vaccine (3rd booster), which was officially approved July 2022 but practically vaccination started beginning of October 2022 and only a tiny fraction of the eligible population took it.
*During the bivalent vaccine deployment was is a difference in the ratio of IS in vaccinated vs. unvaccinated, it was started earlier. See below.
Ischemic Stroke and Covid-19
One possible cause is Covid-19. Ischemic stroke following COVID-19 is a known neurological complication. In Israel 2020, 425,525 Covid-19 cases were detected (roughly 5% of total pop.) with a wide spectrum of severity, and assumably several times more undetected cases. Yet there was no significant rise in IS cases during 2020. Therefore the impact of Covid-19 on IS should be questioned.
Vaccine-related Ischemic Stroke
Two attributes of the mRNA vaccine make it a possible factor for increased risk of IS:
mRNA vaccines are associated with thrombosis (blood clots) (5) (6)
mRNA vaccines are associated with myocarditis and pericarditis, both of which are associated with arrhythmia (irregular heartbeats), which is a known risk factor for ischemic stroke (7) (8)
In our case those two factors, Covid-19 and vaccines, are intertwined:
The vaccine campaign overlapped the major Covid-19 waves
mRNA vaccines increase the risk of Covid-19 infection (9) (10) (11)
Due to limited data and to the Healthy Vaccinee Effect we could not reliably assess the absolute risk of IS in vaccinated and unvaccinated individuals. Instead, we compared IS cases in vaccinated vs. unvaccinated during 2021-2022. We focused on age 40 and above (below 40 there are few cases of IS which will not affect the total), and we applied a 5-month moving average filter, which is a tradeoff between removing excessive noise from the graphs and maintaining the trends. The graph starts on March 2021 and ends Oct. 2022 due to the 2-month extra margin required by the 5-month moving average calculation.

The left part of the graph (Orange background) depicts the first months of the vaccination rollout, during which Vaccinated and Unvaccinated group sizes changed. By the end of April 2021 the vast majority of the population was vaccinated (regardless of the number of doses), and due to the moving average filter, the graph settles by June 2021.
In order to compare the bottom Blue line (IS in Unvaccinated) to the Red line (IS in Vaccinated), we adjusted the Unvaccinated graph by multiplying the case numbers by a factor of 2.2 (vertically scaling the graph), to compensate for the difference in group sizes. For the sake of comparison we shifted the graph up to overlap the Vaccinated graph.
By simply adjusting the scale, the graphs fit almost perfectly from July 2021 through Feb. 2021 (Yellow background). This is despite a Covid-19 wave (Aug.-Dec. 2021) and the first booster (Aug.-Nov. 2021).
On March 2022 (Grey background) some unknown new factor came into play. While the Unvaccinated IS events kept subsiding, the Vaccinated numbers started climbing again. Beginning March 2022, the constant rise in the Vaccinated IS case numbers, together with the fact that this group is much larger, are the obvious causes for the rise in Total IS cases in 2022, as can be seen in the Total Cases line (Yellow line).
The difference between the two groups is clear - one group got vaccinated, the other did not. A possible explanation for the timing of March 2022 is a medical intervention: 770,000 second-booster doses given January-March 2022. The vaccination campaign continued beyond March, and IS event numbers in the vaccinated kept climbing (with or without a causal relation). Currently, the total second-booster doses given in Israel is 920,000 .
*We refuted a possible bias/mistake of newly vaccinated persons around March 2022. Throughout 2022 only 0.25% more people took the first dose (i.e. newly vaccinated).
Why didn’t the first booster cause a similar rise in IS cases? Some possible explanations are changes in the vaccine, a defective batch, or improper storage & handling. This could also explain the formerly-mentioned CDC/FDA safety signal that appeared and later decreased. Divergence in batch safety has already been demonstrated in Pfizer’s BNT162b2 vaccines.
Conclusion
In order to investigate the cause for the rise in ischemic stroke, it is imperative to distinguish between two known risk factors: Covid-19 and Covid-19 vaccines (other factors should also be considered).
Our analysis points to the vaccine, not the disease, as the main factor, based upon 2020 IS rates vs. 2021-2022, and upon comparison of IS cases in vaccinated/unvaccinated.
We did not find data to support the common conclusion that Covid-19 significantly increases the risk of ischemic stroke.
Unbiased research is required to further understand the effects of those two factors on the risk of ischemic stroke, to identify specific risk groups (certain age groups, gender, different sub-types of ischemic stroke).
In addition, when weighing the risk-benefit of the vaccine, one must take into account the personal decision and the Rechallenge effect: If a person decides to get vaccinated they will 100% get vaccinated, most likely with multiple doses (hence Rechallenge - increased risk of adverse events with each dose). With Covid-19, a person may or may not get infected or reinfected - the risk of infection is always lower than 100% and can partly be controlled by a person’s lifestyle.
Reference
Ischemic stroke
Ischemic stroke occurs when the blood supply to part of the brain is interrupted or reduced, preventing brain tissue from getting oxygen and nutrients. It is usually caused by a blood clot that blocks or plugs a blood vessel in the brain. Symptoms include sudden numbness or weakness of the face, arm, or leg, especially on one side of the body, confusion, trouble speaking or understanding, trouble seeing in one or both eyes, trouble walking, dizziness, loss of balance or coordination, and severe headache with no known cause. Treatment may include medications to dissolve blood clots, procedures to remove blood clots, and surgery to repair blood vessels.
Source files
FOIA Response from Clalit Health Fund
{kind=link}
ICD-9 codes used:
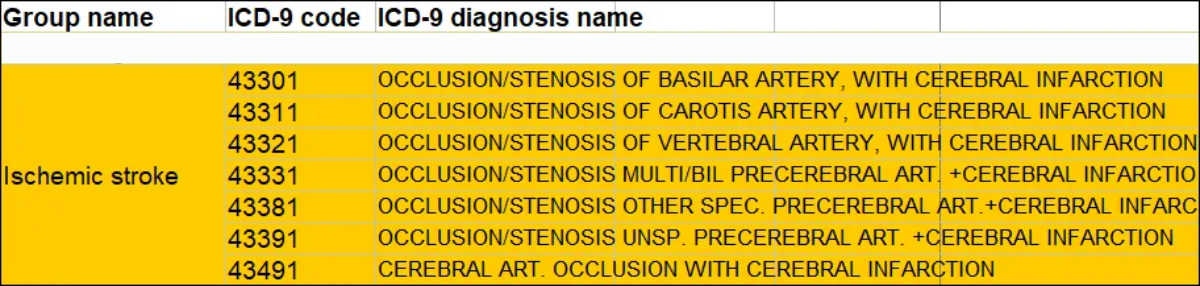
... and this.
‘Spikeopathy’: COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA
https://www.mdpi.com/2227-9059/11/8/2287
Biomedicines 2023, 11(8), 2287; https://doi.org/10.3390/biomedicines11082287
Accepted: 24 July 2023 / Published: 17 August 2023
-
"Abstract
The COVID-19 pandemic caused much illness, many deaths, and profound disruption to society. The production of ‘safe and effective’ vaccines was a key public health target. Sadly, unprecedented high rates of adverse events have overshadowed the benefits. This two-part narrative review presents evidence for the widespread harms of novel product COVID-19 mRNA and adenovectorDNA vaccines and is novel in attempting to provide a thorough overview of harms arising from the new technology in vaccines that relied on human cells producing a foreign antigen that has evidence of pathogenicity. This first paper explores peer-reviewed data counter to the ‘safe and effective’ narrative attached to these new technologies. Spike protein pathogenicity, termed ‘spikeopathy’, whether from the SARS-CoV-2 virus or produced by vaccine gene codes, akin to a ‘synthetic virus’, is increasingly understood in terms of molecular biology and pathophysiology. Pharmacokinetic transfection through body tissues distant from the injection site by lipid-nanoparticles or viral-vector carriers means that ‘spikeopathy’ can affect many organs. The inflammatory properties of the nanoparticles used to ferry mRNA; N1-methylpseudouridine employed to prolong synthetic mRNA function; the widespread biodistribution of the mRNA and DNA codes and translated spike proteins, and autoimmunity via human production of foreign proteins, contribute to harmful effects. This paper reviews autoimmune, cardiovascular, neurological, potential oncological effects, and autopsy evidence for spikeopathy. With many gene-based therapeutic technologies planned, a re-evaluation is necessary and timely."
-
Keywords: spike protein; pathology; transfection; biodistribution; lipid-nanoparticles; autopsy; inflammation; pharmacovigilance; COVID-19; mRNA vaccines
---
I wonder, what kind of warning signals we need to stop the "booster" and the "spike" in death ...
I may add some add. color to the "riddle":
-
FDA amended EUA for COVID bivalent mRNA technology booster (April 18th) (Pfzier-BioNTech & Moderna for original & BA4/BA5 clades); then CDC’s ACIP advisory group met April 19th, 2023
https://dailyclout.io/fda-amended-eua-for-covid-bivalent-mrna-technology-booster-april-18th-pfzier-biontech-then-cdcs-acip-advisory-group-met-april-19th-2023/
April 25, 2023 - by Dr. Paul Alexander
---
Ahead of time however:
-
Brain injuries after COVID vaccination
https://colleenhuber.substack.com/p/brain-injuries-after-covid-vaccination
"There are back door routes to the brain. COVID vaccine developers have traversed a path through those doors. And they knew they had entered the brain by November 2020, before the vaccine rollout."
10.04.2023 - DR. COLLEEN HUBER
---
... and later then:
Neurological symptoms after COVID-19 vaccination: a report on the clinical presentation of the first 50 patients
https://link.springer.com/article/10.1007/s00415-023-11895-9
https://doi.org/10.1007/s00415-023-11895-9
Published 29.07.2023
---
This might have to be considered as well:
-
Amyloidogenesis of SARS-CoV-2 Spike Protein
https://pubs.acs.org/doi/10.1021/jacs.2c03925
https://doi.org/10.1021/jacs.2c03925
17.05.2022
-
Follow up on DNA contamination of COVID-19 injectable products
It's worse than originally thought based on new results...
https://jessicar.substack.com/p/follow-up-on-dna-contamination-of
March 9, 2023 - Jessica Rose